- Ginecoweb got a brand new image!
- Women´s health for all!
Anatomy and localization
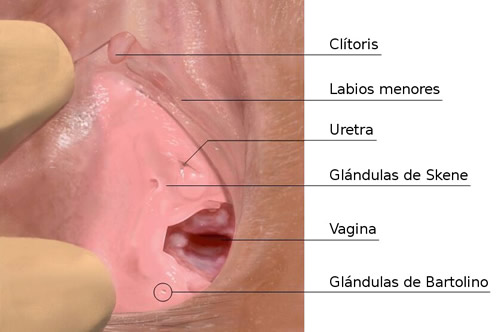
In this real photo only holes in ducts can be seen, the glands are not nor can be felt due to the fact that they are normal.
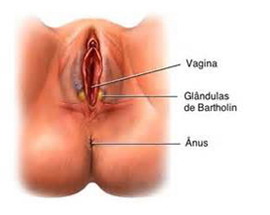
On this scheme you can see in their anatomical location:
And with a cyst or abscess:


Treatment
Puncture drainage: it punctured and drained the gland, anesthesia is not used.

Drainage by incision: I use a blade of knife #11 (Lancet) and pierced the gland without using local anesthesia since infiltrating the area with local anesthetic is extremely painful. Drilling is practically painless and drainage occurs quickly obtaining immediate symptomatic improvement.

Marsupialization: gland is surgically opened and drained the contents are stitched edges to keep it open to the outside and ensuring its drainage. The recurrence rate is low for this procedure. Practiced in the operating room.
Glandular Exceresis: the total number of the affected gland is surgically removed.