- Ginecoweb got a brand new image!
- Women´s health for all!
Endometriosis is a chronic disease which is manifested by the appearance of endometrial tissue outside their normal anatomical location: uterine inside. The endometrial tissue is implanted outside the uterus in the pelvic cavity, fallopian tubes, ovaries, abdominal injury, cervix, vagina, etc., and to respond to the stimulus menstrual normal (bleeding) generates an inflammatory lesion which leads to the emergence of local pain, adhesions and infertility due to injury of the pelvic organs, especially the fallopian tubes and ovaries.
The problem
Endometriosis is one of benign diseases most common in women in the reproductive age, affecting up to 1 in 5 women (20%), and is a very important cause, if not the most common, chronic pelvic pain and female infertility.
The theory most accepted at the origin of this disease is menstrual bleeding through the fallopian tubes into the interior of the pelvic cavity in what is known as retrograde menstruation (anterograde menstruation is that we all know as the bleeding (vaginal monthly) in susceptible patients whose body allows that menstrual tissue with endometrial cells implant abnormally in any location or pelvic organ.
Now, to have cells and endometrial tissue which responds to the menstrual cycle have menstrual bleeding in locations not prepared for it and it will generate an inflammatory reaction in the affected tissues that would explain the symptoms and complications caused by the disease.
Endometriosis is not cancer, is it a contagious disease, or is associated with any infectious organism. It isn't fatal but it can significantly alter the life of a woman who is not controlled adecuadamene.
What are the symptoms of endometriosis?
The symptom most frequently reported is pelvic pain that has some very special characteristics: menstrual pain (dysmenorrhea) increasingly more intense or of first occurrence in a woman who had never before menstrual pain, pain with relations sexual (dyspareunia), pain during gynecological touch, chronic pelvic pain, rectal pain, and unspecified urinary discomfort.
An important part of women with endometriosis will not manifest no symptoms and the disease it could manifest inability to achieve a pregnancy. This is because that the adhesions, scarring and fibrosis caused by endometriosis can deform, obstruct or alter the normal architecture of the fallopian tubes, preventing the normal process of fertilization as well.
Heavy menstrual bleeding (hipermenorrea) is also often caused by infiltration endometriosica of the uterine wall and their inability to proper contraction which limits menstrual bleeding (it's called Adenomyosis).
Moreover, some patients report discomfort pelvic unspecific associated with bloating gas and intestinal discomfort, rectal pain and urinary discomfort by intestinal endometriosis, adhesions and bladder injuries.
In addition, severe menstrual pain (dysmenorrhea) and back pain, flanks and legs due to nerve irritation caused by implants in the sacral region.
How do we diagnose it?
Medical history gathered with the patient's symptoms and data found by physical examination of the doctor generates the clinical suspicion about the presence of endometriosis. The background and the manifestations of pelvic pain and infertility are very useful for diagnostic exercise
Gynecological touch can put of manifest exquisitely painful points or even the presence of painful pelvic tumors (ovarian endometriomas).
Transvaginal ultrasound can identify indirect data of disease as well as features of ovarian endometriosis (cysts in frosted glass) images which in practice are referred to as chocolate cysts by its visual appearance
The diagnostic method par excellence is the pelvic examination to direct vision via laparoscopy Diagnostica/operatoria, instrument that not only allows the diagnosis of the severity of the disease but also allows the taking of tissue samples for histo-pathological diagnosis and correction of the susceptible lesions by surgical treatment: liberation of adhesions and scarring, release of the fallopian tubes, ovarian Cystectomy, removal of pelvic endometriotic implants between other
Definitive diagnosis to justify prolonged by endometriosis treatments must be tissue biopsy and histopathological diagnosis. Gynecologic laparoscopy is the diagnostic method and therapeutic choice.
How can we treat endometriosis?
Treatment options depend on the degree of spread of the disease, reproductive desire of the patient and disability that pain the patient manifests
The best immediate treatment is the pelvic surgery by laparoscopy that as well as allowing us obtaining a tissue sample to make accurate diagnosis allows us to determine the stage of the disease (decision for therapeutic and prognostic) and recover surgically the pelvic anatomy. The advantage of this method in comparison to traditional open surgery is the rapid recovery and poor handling of the pelvic organs without that there isn't a large wound that can complicate or generate an undesirable aesthetic effect
Hormones and anti-hormonal drug are helpful and the element of long-term control of the disease and the contributing factor of the surgical management of the disease. It ranges from common oral contraceptive use to the use of substances that cause menopause-like States.
The most natural and significantly effective treatment that exists is the pregnancy of women affected by this disease. It is a free treatment of 9-month capable of stunt implants and endometriosicas tumors.
Recently it has been determined that the use of hormonal intrauterine devices as the Mirena are very effective in controlling the disease uterine endometriosica (Adenomyosis) and of the endopmetriosis pelvic, providing a treatment regimen quite economic, involuntary and nearly free of side effects.
Endometriosis cures?
Lol Endometriosis is a chronic disease that depends on the hormonal status of women suffering from it, so while there is sexual hormonal function disease will continue to present. Menopause puts an end to its existence but leaves its consequences (adhesions, painful anatomical alterations). Pregnancy and lactation uina generated great improvement that has a tendency to last for some months or years after completed.
In the end, the patient suffers from a chronic condition that can be properly handled but that requires regular monitoring and prolonged medical treatment.
Surgery should be used in the initial stages for the correct diagnosis but thereafter should be avoided as much as possible since it could lead to unnecessary mutilation and distortion of the pelvic Anatomy as well as alteration of the female hormonal function by injury Ovarian surgery.
There is some relationship between the ovarian endometriosis and ovarian cancer, always indicated surgery as a preventive treatment for ovarian cancer.
What is the prognosis of infertility?
Most of the affected patients may develop following natural or advanced methods according to the particular conditions of the disease of the patient (Stadium of endometriosis), male factors associated with your partner and other associated factors that it could limit the female fertility.
Older lower fertility and longer time exposed to the disease, so, we recommend pregnancies at early ages, or at least not excessively prolong the reproduction. The age and the time of exposure, especially in the absence of adequate medical control of the disease, are our worst enemies reproductive.
Ovarian endometriosis
-

- Imagen ecográfica en vidrio esmerilado de un ovario, acumulación de sangre en el ovario.
Adenomyosis: a particular endometriosis
Adenomyosis is a form particularly of endometriosis endometriotic implants that are located in the thickness of the uterine muscle (Myometrium). This alters uterine architecture and function. The uterus is more voluminous expected, tender and painful. The patient manifests abundant menstrual bleeding and pain.
-

- En esta imágen se observa un útero globoso que se deforma por la presión del instrumental; además, se ven los implantes endometriósicos en la superficie uterina.
-

- El útero está infiltrado por glándulas endometriales (imágenes redondeadas) en el tejido muscular y una amplia reacción inflamatoria (imágenes puntiformes múltiples alrededor de las glándulas)
-

- En ésta imágen ecográfica se aprecia un útero globoso y miometrio heterogéneo. Durante el estudio se puede desencadenar molestia local cuando se ejerce presión uterina con el transductor vaginal
Surgical vision
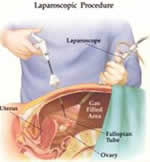
Laparoscopy in endometriosis:
-

- Detalle de un implante endometriosico. Estos se documentan, se toma una muestra para diagnóstico histopatológico y luego se fulguran con electricidad.
-

- Quiste de chocolate: endometrioma ovárico con el característico color marrón a negro que le da su nombre.
You have access to the pelvis in a way minimally invasive, with less collateral surgical lesion, excellent control of the disease and rapid clinical recovery with laparoscopy. The method is based on the abdominal entry of fine instruments guided by high-resolution video. They enter between 3 and 4 abdominal ports, one in the navel (invisible) and 2 on each side of the abdomen below the navel (less than 10 mm).

In the operating room, we continue the intervention through the use of TV monitors strategically placed so that all personnel have appropriate image.

To breathe air into the abdomen organs separate giving us visual field for carrying out the operations indicated in the pelvic organs.
Given that wounds are very small and that the internal manipulation is minimum (minimally invasive surgery) postoperative pain and recovery is low and fast, respectively.

Due to some cases of inadvertent castration in the woman who has suffered several interventions because of their endometriosis, we have adopted a scheme very conservative, especially if it's ovarian endometriosis, to prevent the removal of ovarian tissue. We accept greater residual disease and manage the remaining schemes hormonal or antihormone to avoid multiple interventions and the risk of castration.
Vicariante hemorrhage: a very rare case

Primary umbilical endometriosis
Menstruation Vicariante: menstrual bleeding in organs other than the uterus. Patient with no previous surgery bleeding menstrual and umbilical monthly. There have been cases of lacrimal endometriosis which would explain cases of
Famous endometriosis
Marilyn Monroe (1926-1962), famous actress from the 1950s, perhaps unknown to recent generations, suffered severely due to endometriosis, such was the seriousness of his condition that destroyed their marriages (3), their desire to have babies, career acting in Hollywood and eventually his life.
It was intervened on several occasions by the disease. In this photo you can see the scar left by the removal of the gallbladder, the only intervention of the 7 that you had, that was not related to endometriosis. Pelvic scarring are cross-cutting and are not seen in this picture.
