- Ginecoweb got a brand new image!
- Women´s health for all!
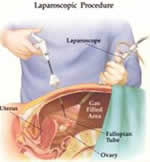
You have access to the pelvis in a way minimally invasive, with less collateral surgical lesion, excellent control of the disease and rapid clinical recovery with laparoscopy. The method is based on the abdominal entry of fine instruments guided by high-resolution video. They enter between 3 and 4 abdominal ports, one in the navel (invisible) and 2 on each side of the abdomen below the navel (less than 10 mm).

In the operating room, we continue the intervention through the use of TV monitors strategically placed so that all personnel have appropriate image.

To breathe air into the abdomen organs separate giving us visual field for carrying out the operations indicated in the pelvic organs.
Given that wounds are very small and that the internal manipulation is minimum (minimally invasive surgery) postoperative pain and recovery is low and fast, respectively.

Training
Ethicon/Johnson, Ircad, Winners Project institutions have developed programmes Basic, intermediate and advanced which guarantee the correct learning of all areas related to the efficient, low risk and control laparoscopic surgery of complications:
- They induce the anatomical study, physiological and pathophysiological of surgical specialty.
- They oblige the knowledge and proper use of the instruments and operative energies to optimize procedures and avoid accidents.
- They promote the use interface of the human and material resources that surround the surgery.
- They oblige the acquisition of new skills, psychomotor, ergonomics and efficiency.
- Require the surgeon to be responsible at all stages that surround the surgical Act.
- They emphasize the need for recurring regular and formal training to maintain and extend skills.
My simulators: perfect practice makes perfect.
TASKit of Ethicon, Johnson & Johnson. Courtesy of their representatives in Caracas. It is my portable practice team.


Endotrainer de el Dr Eduardo Troconis. Fixed in my office
Surgery may not be unpredictable. Surgeons must control everything, follow the rules and provide strategies, because there is no room for uncertainty.
Surgeons have to train to simulate difficult situations and confront them with success in reality.