The truth is that they are almost always of ovarian origin, most of them benign and relatively easy to diagnose and treat
Women in reproductive age will be the largest number of ovarian tumours: functional benign, endometriotic and occasionally solid trend or frankly malignant.
You can start intervention via laparoscopic – to assess the tumor and pelvic environment – and then go to open surgery for the injury through an abdominal incision of appropriate size.
Frequent tumors
Diagnosed as such when the "real" ovaries can be seen in the vicinity.
This is the main cause of ectopic pregnancy
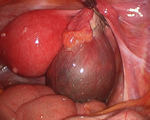
Endometriomas: endometriosis is a benign disease most common in women in the reproductive age, affecting up to 1 in 5 women (20%), and is a very important cause, if not the most common, chronic pelvic pain and infertility.
They are almost invariably benign and grow by compressing the healthy ovarian tissue. They are really nasty cut but are beautifully benign in their behavior.
Associated with ovarian cancer radical surgery has proven to be highly efficient and even better than traditional open surgery, is basically more efficient, less traumatic, and due to the magnification of the image allows a better removal of lesions metastatic and typical lymph node dissection of the oncological surgery.
Update on early detection of Ovarian Cancer
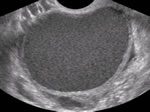
According to the findings of an article published in the Lancet, December 2015, will start the measurement of a tumor marker, CA125, annually in all women over 50 years, in conjunction with the study of transvaginal ultrasound that is routine in the query. You must be in the same laboratory annually and their values followed in time. Expected a reduction of 15% (over the 14 years of study) in ovarian cancer mortality using this modality.
Publication of IOTA (International Ovarian tumour Analysis), simple rules for simple Diagnostics and high sensitivity of the cancer of ovary (ultrasound) transvaginally. IOTA Summary Paper 2013
Determination of malignancy (Imaging) ultrasound
{kind=link}
Risk of malignancy IOTA-ADNEX calculator
Salpingectomy opportunist
Since 2010 is is suggesting the Elimination of the fallopian tubes as a method to decrease the risk of Ovarian Cancer (cancer of the ovary, fallopian tubes, and local peritoneum) when it is desirable to leave the ovaries in place for women at average risk, bass, of cancer Ovarian. This began to study since it is known that the tubal ligation (surgical sterilization) reduces the risk by 10-20%; the removal of fallopian tubes during hysterectomy or sterilization method reduces the risk to 40-50%. We offer this procedure to patients undergoing hysterectomy since it helps us to decide to leave the ovaries and fallopian tubes removed. This seems to be that, in terms of prevention, it is best to remove the tubes to the ovaries, which does not affect the overall health of the women by the surgical castration of the removal of the ovaries.
Women with high risk must be subjected to total removal of ovaries and fallopian tubes; these patients are usually positive for the BRCA1 and BRCA2 genes mutations; risk of ovarian cancer of 40-60% and 20 to 30%, respectively.
Abscess tubal

Teratoma, dermoid cyst

Hair, fat, bones, teeth, glands… teratoma. (In most cases) benign tumor

Functional cyst
The most frequent of the ovarian cysts, the functional is occasionally operated